


History - 14yrs old boy with c/o headache, decreased vision in left eye, weight gain and excessive sleepiness.
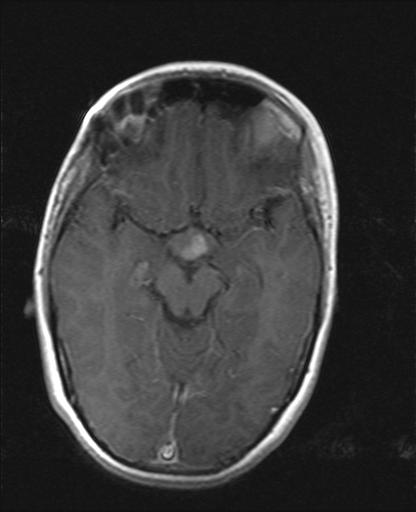
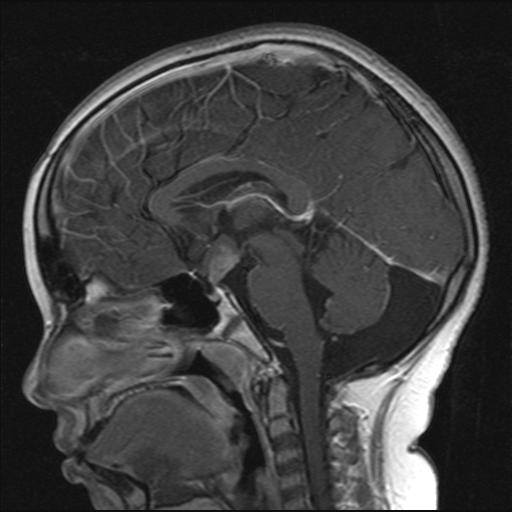
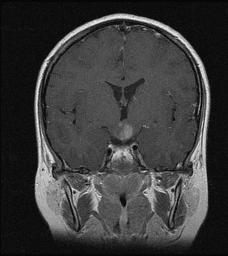
Findings - Enhancing lesion noted involving the left hypothalamus.
Findings - Enhancing lesion noted involving the left hypothalamus.
Hypothalamic glioma
This tumor belongs the group of Juvenile pilocytic astrocytomas. Juvenile pilocytic astrocytomas occur more often in children and young adults. They are the most common astrocytic tumors in children, accounting for 80-85% of cerebellar astrocytomas and 60% of optic gliomas.
These tumors are usually discrete, indolent lesions associated with cyst formation. The cysts can be unilocular or multilocular, with an associated tumor nodule.
Juvenile pilocytic astrocytomas are further categorized as :
1. Supratentorial juvenile pilocytic astrocytoma.
2. Optic nerve and optic chiasm hypothalamic gliomas.
3. Posterior fossa juvenile pilocytic astrocytoma
The most common site of occurrence of juvenile pilocytic astrocytoma is in the cerebellum.
Optic pathway gliomas (OPGs) account for approximately 5% of all brain tumors and 10% to 15% of supratentorial tumors in children. The tumor can arise anywhere along the optic pathway, from just behind the globe to the occipital cortex. The diagnosis of OPG also covers cases of hypothalamic chiasmatic glioma, in which it is difficult to distinguish the site of origin. In children, OPGs are almost always low-grade astrocytomas .
People with neurofibromatosis -1(a hereditary condition) are at increased risk for this type of tumor in particular but It is unclear whether OPG associated with neurofibromatosis (NF) is a distinct entity from non–NF-OPG. The NF1 gene has been located at chromosome 17, and its protein product, Neurofibromin, characterized. The association of both benign pilocytic and diffuse astrocytomas with NF points to a role for the NF1 gene in the pathogenesis of gliomas in these patients. Neurofibromin is believed to act as a tumor suppressor.
MRI Findings :
Optic chiasm hypothalamic gliomas cannot be separated by their site of origin and are considered as a single entity. On T1-weighted images, the signal intensity is low. On T2-weighted images, the signal intensity is generally increased. The T2 signal intensity increase may extend as far as the optic radiations, but it is not correlated directly with the presence of tumor. Enhancement is similar to that on CT scans. Fat-saturated T1-weighted post contrast MRI of the intra orbital optic nerves is a sensitive method for demonstrating the tumor.
A study published in AJNR, 2001 gives following differences between NF OPG and non NF OPG.
1.In the patients with NF, the most common site of involvement was the orbital nerve. The tumor was smaller than in the non-NF patients, the original shape of the optic pathway was preserved, and cystic components were uncommon. In the non-NF group, the chiasm and hypothalamus were the most common sites of involvement, the tumor was mass like, and cystic components were frequently seen, as was extension beyond the optic pathways.
2. The non-NF patients were referred for examination because of their symptoms, whereas NF patients were asymptomatic at the time examination .The smaller dimensions and the relative sparing of the hypothalamus in the NF patients may account for this finding. The lag between the onset of symptoms and the imaging study was much longer in the non-NF group (up to 4 years), whereas NF patients were examined immediately.
3. Hydrocephalus as a presenting symptom was found exclusively in the non-NF group. Precocious puberty was associated only with NF. A significant correlation was found between hypothalamicinvolvement and the occurrence of endocrinologic symptoms (such as failure to thrive and precocious puberty) and signs of increased intracranial pressure. Interestingly, orbital involvement did not correspond to visual symptoms, possibly because infants and even young children tend not to complain of visual disturbances.
4.One of the most striking features differentiating NF-OPG from non–NF-OPG is the long-term behavior of the tumor. The majority in the NF remained stable whereas in the non-NF group, there was a clear propensity for growth.
Differential diagnosis for Optic nerve and optic chiasm hypothalamic gliomas include:
Craniopharyngioma
Meningioma
Hamartoma
Germinoma
Histiocytosis
Sarcoidosis
Craniopharyngioma
Meningioma
Hamartoma
Germinoma
Histiocytosis
Sarcoidosis