


Corpus callosal agenesis with nodular heterotopia
Corpus callosum is the largest cerebral commissure connecting neocortical areas and develops between 12 to 20 weeks of gestation. The most anterior portion, the rostrum, develops first and is followed by the genu, body and splenium.
In agenesis of corpus callosum, commissural fibres do not cross the midline instead thick bundles of intersecting fibres called Probst bundles are seen which lie along the super medial aspect of the lateral ventricles and the third ventricle may sometimes be displaced upward. In most cases there is a stable, non-progressive dilatation of the caudal portion of lateral ventricles.
In agenesis of corpus callosum, commissural fibres do not cross the midline instead thick bundles of intersecting fibres called Probst bundles are seen which lie along the super medial aspect of the lateral ventricles and the third ventricle may sometimes be displaced upward. In most cases there is a stable, non-progressive dilatation of the caudal portion of lateral ventricles.
Callosal dysgenesis may be considered in three distinct categories: callosal agenesis, hypogenesis and hypoplasia.
In callosal agenesis, the corpus callosum is completely absent.
In callosal hypogenesis (partial callosal agenesis), the corpus callosum is variably formed. The splenium and rostrum are always missing, the genu and the body are present to varying degrees.
Callosal hypoplasia refers to a corpus callosum that is completely formed but focally or generally small in size; this usually occurs in the setting of cerebral cortical dysgenesis, with poor development and/or abnormal myelination of crossing callosal fibers.
Imaging Findings
1. Absence of corpus callosum
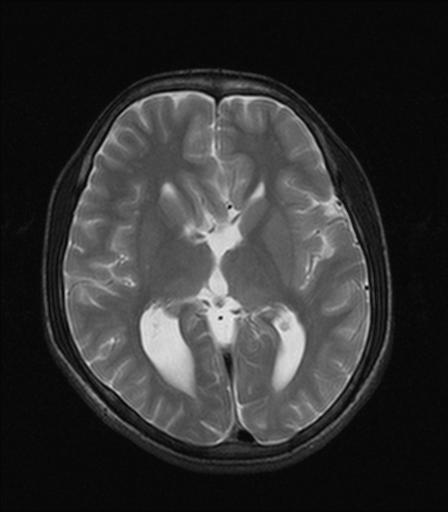
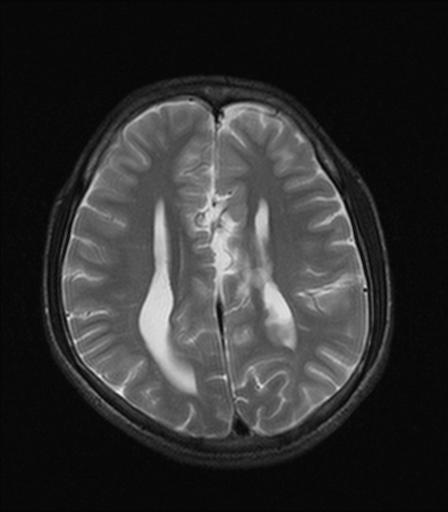
2. Widely place, parallel, non-converging lateral ventricles.
3. Small pointed frontal horns with disproportionately enlarged occipital horns (colpocephaly).
4. Longitudinal white matter tracts (Probst bundles) indent superomedial lateral ventricles.
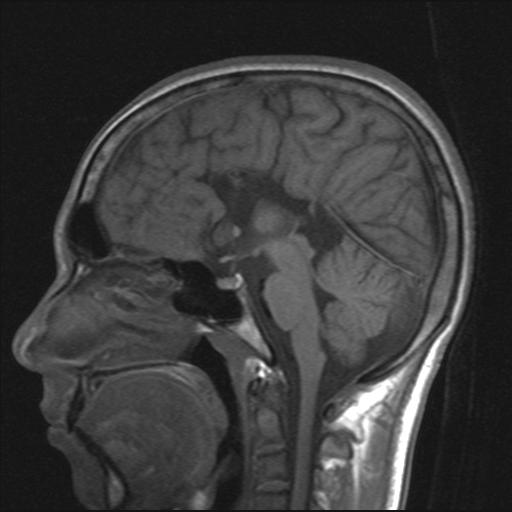
5. High riding third ventricle open superiorly to interhemispheric fissure, with or without dorsal cyst.
6. Radial, spoke like orientation of gyri.
Loss of the supporting function of the corpus callosum results in upward bulging of the roof of the third ventricle into the interhemispheric fissure. This upward herniation of the distended third ventricle is generally referred to as the interhemispheric cyst, but it should not be confused with a true dorsal or arachnoid cysts of the interhemispheric fissure found in some cases of callosal agenesis. Extraaxial cysts associated with callosal agenesis should be differentiated from intraaxial midline cysts such as porencephalic cyst, dorsal cyst with holoprosencephaly, simple upward extension of the lateral ventricle in corpus callosum agenesis.
Types of midline cyst formation
Raybaud and Girard suggest that there are 3 types of midline cyst formation in association with agenesis or hypogenesis of the corpus callosum.
Type 1 is a large midline cyst that communicates with third ventricle and the lateral ventricles.
Type 2 is similar to type 1, associated cortical anomalies (eg, polymicrogyria, gray matter heterotopia, schizencephaly) are present.
Type 3 involves complex, multilocular cysts that are asymmetric and independent of the ventricles. Cortical malformations are uncommon. With large cysts, the ipsilateral lateral ventricle may be compressed, and the contralateral ventricle may be obstructed and enlarged (hydrocephalus).
Clinical presentation
The clinical manifestations of callosal agenesis can be described under 2 headings: nonsyndromic and syndromic.
Nonsyndromic forms are the most common. An unknown, though probably small, proportion of patients are completely asymptomatic, or more commonly, their condition is incidentally discovered during neuroimaging. Patients may present with mental retardation or delayed development, seizures, and cerebral palsy. Macrocephaly may be seen due to hydrocephalus sometimes associated with interhemispheric cysts.
It has been associated with several syndromes Andermann Syndrome (peripheral neuropathy with corpus callosum agenesis). Aicardi Syndrome (infantile spasms, ocular anomalies and agenesis of corpus callosum), Shapiro's syndrome (paroxysmal hypothermia with agenesis of corpus callosum) and sporadically with Dandy Walker syndrome, fetal alcohol syndrome, Leigh's syndrome, Arnold Chiari II syndrome.
Other anatomic abnormalities in patients with ACC include hydrocephalus; cephaloceles; and neuronal migration disorders such as lissencephaly, schizencephaly, gray matter heterotopias, pachygria, and polymicrogyria.
Diagnosis
USG
Antenatal diagnosis of ACC is possible from about 20 weeks' gestation.
The typical ultrasound features are absence of corpus callosum and cavum septum pellucidum, increased separation of the lateral ventricles. There is marked separation of the slit like horns of the lateral ventricles, dilatation of the occipital horns creating a typical 'rabbit's - ear' appearance and upward displacement of the third ventricle.
MRI
MRI is currently the imaging procedure of choice in infants and children with ACC, permits confident diagnosis of ACC and its associated anomalies, especially neuronal migration anomalies or atypical forms of holoprosencephaly. Sagittal T1-weighted images clearly demonstrate the exact extent of callosal dysgenesis.
Prognosis: the corpus callosum is phylogenetically a recent structure, and its absence is not lethal. The diagnosis if apparently isolated fetal agenesis of corpus callosum (in the absence of sonographically detectable anomalies) appears to carry an excellent prognosis with an 85% chance of normal developmental outcome and 15% risk of handicap in the form of seizures or other mental disorders.
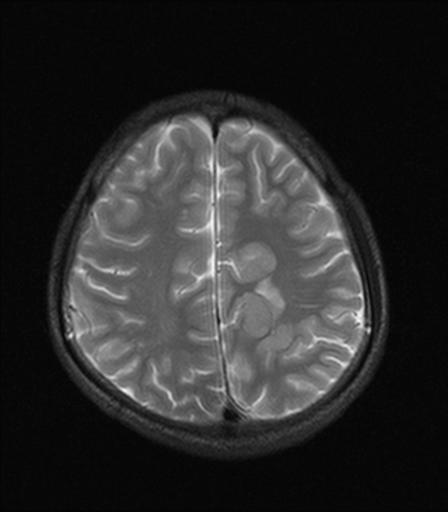
Heterotopias
Gray matter heterotopia are collections of nerve cells in abnormal locations secondary to arrest of radial migration of neurons. Heterotopia can be isolated or associated with other structural anomalies.
Patients with heterotopic gray matter almost always present with seizure disorders. Heterotopia is often divided into three groups: subependymal heterotopia, focal cortical heterotopia and band heterotopia.Patients with band heterotopia often present with “double cortexâ€.
Patients with heterotopic gray matter almost always present with seizure disorders. Heterotopia is often divided into three groups: subependymal heterotopia, focal cortical heterotopia and band heterotopia.Patients with band heterotopia often present with “double cortexâ€.