


Melorheostosis
Melorheostosis is a rare form of mixed sclerosing bone dysplasia that was first described by Leri and Joanny.
Synonyms include Leri type of osteopetrosis , flowing hyperostosis.
The name is derived from the Greek term melos (limb) and rhein (to flow).
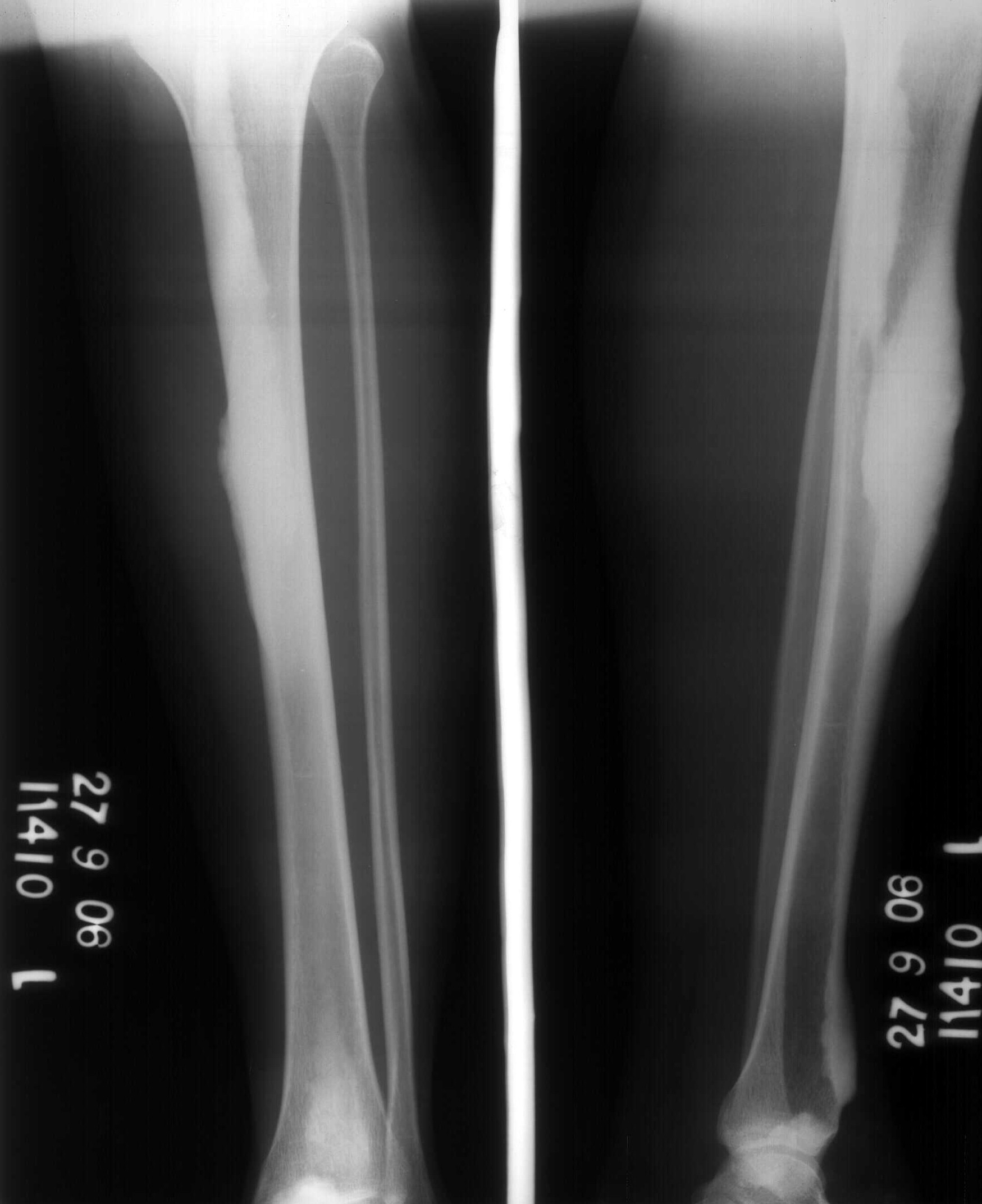
In children, it is characterized by dense linear streaks, mostly in the inner cortex of the affected bones. In adults, irregular ossiï¬cation is seen along the outer cortex, mimicking candle drippings.
The etiology is obscure but Murry and McCreide suggested that an infection associated with nerve roots may be responsible for this rare condition. The lesions follow sclerotomes and myotomes that are supplied by an individual spinal sensory nerve. This may in part explain the monomelic and linear track involvement and distribution of melorheostoses.
Clinical Presentation :
Most authors believe its a congenital entity, most affected individuals do not manifest any symptoms until late adulthood. The onset is insidious with bone hyperostosis progressing through childhood into adult life.
The most common presenting symptom is pain though some cases are found incidentally.
Most of the clinical signs of the osseous dysplasia are associated with ï¬brosis, which is usually the cause for joint stiffness, angular joint deviations, contractures (mostly flexion), and other orthopedic problems.
Skin pigmentation, scleroderma, and tuberous sclerosis-like thickening have been described. In rare instances, melorheostosis has been reported in association with tumors such as spinal column lipomatous osteosarcoma, and soft-tissue lesions such as desmoid tumor. Routine laboratory studies usually are unremarkable.
Radiological features :
Melorheostosis is monomelic and affects one or more contiguous bones.
It is more common in lower extremities and is usually appendicular.
Other possible sites include the skull, spine, ribs, and pelvic bones.
The location is usually diaphyseal.
A well known feature of hyperostotic bone remodeling is its distinctive appearance, resembling wax melting and dripping down one side of a candle. Cortical thickening in a streaked or wavy pattern is the most marked roentgen feature.
In children, the hyperostosis is primarily endosteal; in adulthood, periosteal bone deposition is more dramatic.
The hyperostotic bone protrudes under the periosteum and usually follows along one side of a long bone.
Endosteal involvement may encroach on the medullary space.
Bone masses resembling osteochondromas extend into adjacent articulations.
Involvement of the carpal and tarsal bones resembles the multiple bone islands that are seen in osteopoikilosis.
In pelvis and scapulae (flat bones), the sclerotic bone may be in the form of dense radiations from the joint.
Magnetic resonance imaging (MRI) features of melorheostosis include hyperostosis, which appears as uniform hypointensity on all imaging sequences.
The Tc-99m-MDP three-phase bone scintigraphy image demonstrates moderate to severe increase in tracer in the early and late images, including soft-tissue and blood pool stages of scintigraphy.
Differential diagnosis for this condition includes
1. Osteomyelitis,
2. Reflex sympathetic dystrophy,
3. Neuroï¬bromatosis,
4. Soft-tissue sarcoma, and
5. Metastatic lesions.
Treatment usually is symptomatic, though surgical measures such as osteotomies, excision, capsulotomies, or tendon lengthening often are pursued.