


In 1890s, German pathologist Hans Chiari described a series of anomalies of the caudal cerebellum and brainstem.
In 1891, he described an anomaly consisting of elongated peglike cerebellar tonsils that are displaced into the upper cervical canal through the foramen magnum. This is now designated as the Chiari type Imalformation.
Five years later, he published a further report on a hindbrain anomaly in which the vermis, pons, medulla, and an elongated fourth ventricle were displaced inferiorly into the cervical canal, now known as the Chiari type II malformation.
He also reported a single case of cervical spina bifida associated with herniation of the cerebellum through the foramen magnum, which has since been called Chiari III malformation.
Some authors have added a form of severe cerebellar hypoplasia without displacement of brain through the foramen magnum, the so-called Chiari IV malformation.
CHAIRI I MALFORMATION
Also known as congenital tonsillar ectopia.
Peglike, pointed tonsils displaced into upper cervical canal.
At least 6 mm in the first decade
10-30yrs : 5 mm
30-80yrs : 4 mm
Associated anomalies include mild to moderate hydrocephalus, those of spinal cord like hydromyelia, syringomyelia and syringohydromyelia, and osseous anomalies like basilar invagination and Klippel Feil.
CHAIRI II MALFORMATION
Chiari II malformation includes downward displacement of the medulla, fourth ventricle, and cerebellum into the cervical spinal canal, as well as elongation of the pons and fourth ventricle, probably due to a relatively small posterior fossa.
This disorder is almost invariably associated with myelomeningocele.
I. Osseous changes
1. Lacunar skull or lückenschädel: Almost all patients with Chiari II malformation manifest dysplasia of the membranous bones of the calvarium. This is called lacunar skull (lückenschädel) and appears as clusters of areas of thinning, pits, and fenestrae that are most prominent near the vertex or torcular herophili .The lacunar skull typically persists until the age of 1-3 months and then disappears after approximately 6 months of age, regardless of whether progressive hydrocephalus is present. Subtle calvarial thinning and scalloping may persist into adulthood.
2. Concave clivus and petrous ridge: The posterior aspects of the petrous temporal bones often are concave. The clivus also develops abnormally and often short, with a concave configuration similar to that of the petrous ridges .
3. Small posterior fossa and gaping foramen magnum: The posterior fossa is exceptionally small, and the foramen magnum is larger and rounder than usual.
4. Low-lying transverse sinuses: The internal occipital protuberance is situated just superior to the foramen magnum. The transverse sinuses and torcular herophili are low lying .
II. Changes to the dura
1. Fenestrated falx: The falx almost always shows partial absence, hypoplasia, and/or fenestrations.
2. Hypoplastic tentorium: The tentorium is hypoplastic and attaches to the occipital bone far caudally, just above the foramen magnum.
3. Heart-shaped incisura: The hypoplastic tentorial leaves arise laterally from the low-lying transverse sinuses.
III. Changes to the cerebellum, medulla, spinal cord and fourth ventricle
1. Cerebellar peg: Protrusion of vermis and hemispheres through the foramen magnum (90%) results in craniocaudal elongation of cerebellum behind the spinal cord.
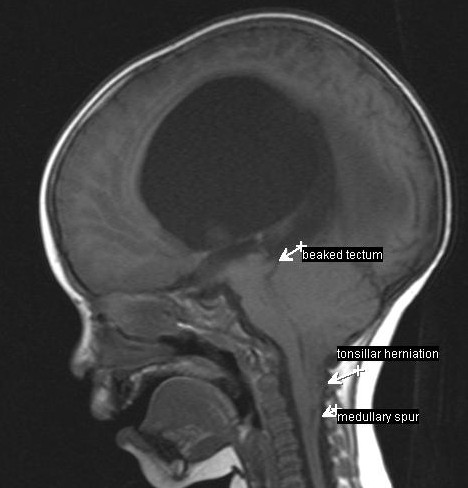
2. Medullary kink: The medulla is kinked inferiorly (75%) and lies dorsal to the cord, which is unable to descend because of competent dentate ligaments.
3. Towering cerebellum or vermian pseudotumor: The cerebellar hemispheres and vermis also extend above the incisura of the tentorium.
4. Cerebellum ‘creeps’ around brainstem : Corners of the cerebellum are wrapped around the brainstem, pointing anteriorly and laterally .
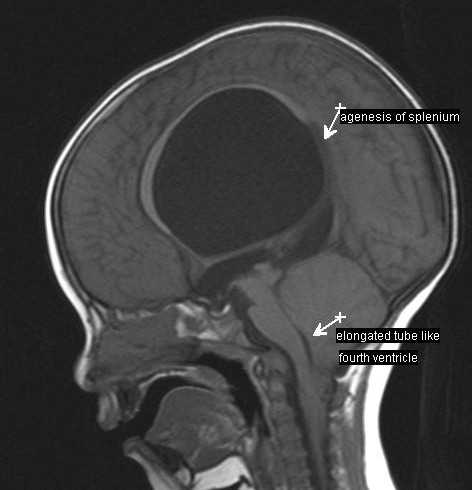
5. Tubelike elongated fourth ventricle: The fourth ventricle is elongated craniocaudally, narrowed transversely, and decreased in anteroposterior diameter.
6. The cerebellopontine cistern and the cisterna magna are obliterated.
7. The combined displacements of the spinal cord, medulla, pons, and cerebellum form a cascade of herniations, each of which compresses all of the tissue in front of it, displacing them anteriorly.
8. In older patients, a wide subarachnoid space may be seen behind a vermis that is deeply grooved at the level of cervical nerve C1. The vertebral artery frequently loops on itself within the cervical canal and passes caudally to the level of cervical nerve C3. The possible cause of this groove may be the pulsatile effect of the vertebral artery on the adjacent cerebellum.
IV. Changes to the midbrain and the third and lateral ventricles
1. Beaked tectum: Variable degrees of fusion of the colliculi and tectum result in prominent beaking and inferior displacement of the tectal plate.
2. Hydrocephalus: Ventricular dilatation is present in 98% of patients, and 90% require a shunt.
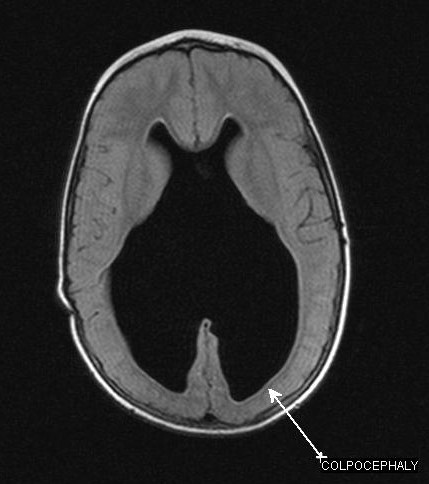
3. Colpocephaly: The occipital horns and atria are often mildly enlarged because of maldeveloped occipital lobes, especially in the presence of a malformation involving the corpus callosum.
4. Prominent massa intermedia: A prominent massa intermedia, herniation of the third ventricle into the suprasellar cistern, and an enlarged suprapineal recess often are seen. Frequently, a large third ventricle is present as well.
5. Approximately one third of infants have a partial block at the level of the ambient cisterns.
Associated anomalies
- Myelomeningocele (88-100%)
- Dysgenesis of corpus callosum (80-90%)
- Obstructive hydrocephalus following closure of myelomeningocele (50-98%)
- Syringohydromyelia (50-90%)
- Aqueductal stenosis (70%)
- Absence of septum pellucidum (40%)
- Contracted narrow gyria (stenogyria; 50%)
- Heterotopias
- Diastematomyelia
- Segmentation anomalies (<10%), incomplete C1 arch
- Malrotation of the posterior arches of C1 and C2.
- Low-lying often-tethered conus medullaris below lumbar nerve L2.
CHIARI III MALFORMATION
In includes hindbrain herniation into a low occipital or high cervical encephalocele in combination with features of the Chiari II malformation.
Cerebellum and occipital lobes are common cephalocele contents.
The herniated tissue is strinkingly abnormal and often non functioning.
CHIARI IV MALFORMATION
Severe cerebellar hypoplasia has sometimes been termed Chiari IV malformation.
Findings in this very rare entity include absent or severely Hypoplastic cerebellum, small brainstem and large posterior fossa CSF spaces.