



Diffuse idiopathic skeletal hyperostosis (DISH)
Paraspinal ligaments undergo degeneration, secondary to attrition, and often ossify. This condition is broadly termed spinal enthesopathy. Physicians recognize 3 syndromes associated with this phenomenon, including (1) Forestier disease (most common; involving anterior longitudinal ligaments) and a more diffuse variant (exhibiting additional extra-axial features) that is termed diffuse idiopathic skeletal hyperostosis (DISH), (2) ossification of the posterior longitudinal ligament (OPLL), and (3) ossification of the vertebral arch ligaments (OVAL).
The etiology of DISH is uncertain. Glucose metabolism imbalance (diabetes), dyslipidemia, and hyperuricemia have been implicated. Following are certain DISH diagnostic criteria:
- Flowing calcifications and ossifications along the anterolateral aspect of at least 4 contiguous vertebral bodies with or without osteophytes
- Preservation of disc height in the involved areas and an absence of excessive disc disease
- Absence of bony ankylosis of facet joints and absence of sacroiliac erosion, sclerosis, or bony fusion, although narrowing and sclerosis of facet joints are acceptable
All three radiographic criteria must be fulfilled to establish a definitive diagnosis of DISH. Each has been chosen to eliminate other spinal disorders, which potentially could be confused with DISH: The first criterion is helpful in separating this condition from typical spondylosis deformans; the second criterion distinguishes DISH from intervertebral (osteo)chondrosis; the third criterion eliminates patients with ankylosing spondylitis.
Occurs more commonly in males (65%) than in females (35%). Usually occurs in persons aged 50-75 years.
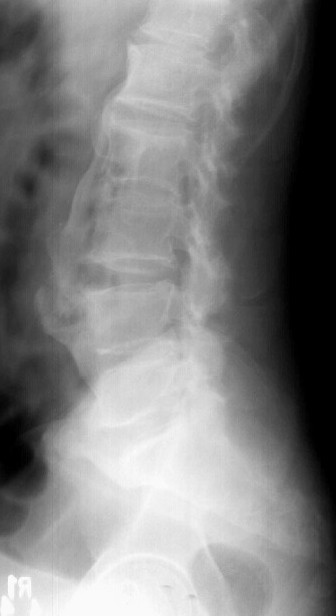
Radiographs of the spine typically demonstrate thoracic spine involvement; however, DISH also can affect the lumbar and cervical spine. DISH is distinguished by the presence of flowing syndesmophytes along, but separated from, the anterior aspect of the vertebral bodies, involving at least 4 levels. The disease begins as fine ossification, 1-to 2-mm thick, but ossification may thicken as much as 20 mm as the disease progresses.