





PULMONARY EMBOLISM ON PLAIN RADIOGRAPH
An initially normal chest X-ray over the time begins to show atelectasis, which may progress to cause a small pleural effusion and an elevated hemidiaphragm.
Chest radiographic abnormalities includes oligemia, vascular redistribution, pleural-based area of increased opacity,pleural effusion, and elevated hemidiaphragm.
1.The Westermark sign is an area of oligemia distal to a large vessel that is occluded by PE. The reduction in local blood volume combined with minimal change in the lung volume causes relative oligemia in the involved lung region. Regional oligemia following PE can be caused either by mechanical obstruction to blood flow or by reflex vasoconstriction, a dilatation of the pulmonary vessels proximal to an embolism along with collapse of distal vessels
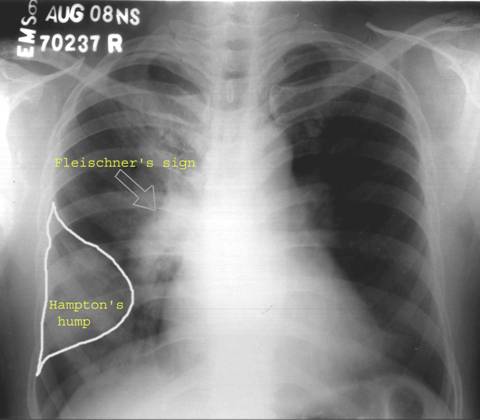
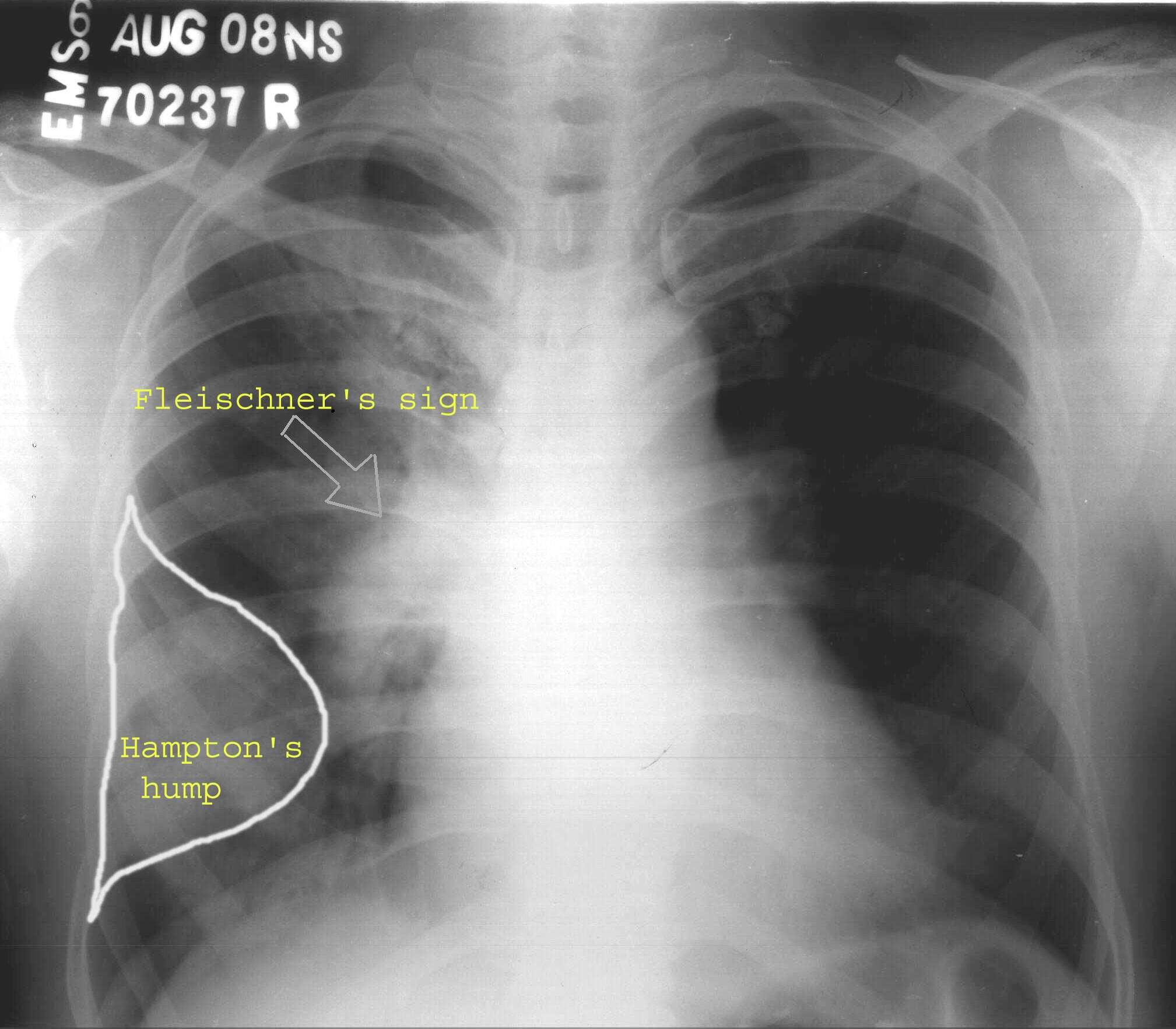
2.The Fleischner sign or a prominent central artery can be caused either by pulmonary hypertension that develops secondary to peripheral embolization or by distention of the vessel by a large clot .
3.Late finding of pulmonary infarction is the Hampton's hump, a triangular or rounded pleural-based infiltrate with the apex pointed toward the hilum, frequently located adjacent to the diaphragm. The Hampton hump appears as a well-defined pleural-based area of increased opacity with a convex medial border; this finding aids in the differentiation of pulmonary infarction from pleural thickening or free pleural fluid.
The main value of the chest radiograph is to exclude diagnoses that may clinically mimic PE and to aid in the interpretation of the ventilation perfusions scan.
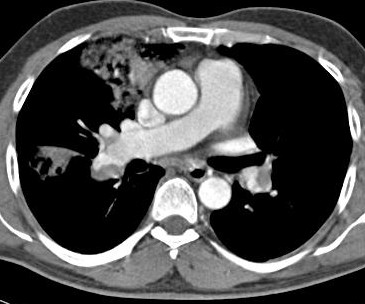
The CT diagnostic criteria for acute pulmonary embolism include the following:
1. Arterial occlusion with failure to enhance the entire lumen due to a large filling defect; the artery may be enlarged compared with adjacent patent vessels .
2. A partial filling defect surrounded by contrast material, producing the “polo mint†sign on images acquired perpendicular to the long axis of a vessel and the “railway track†sign on longitudinal images of the vessel .
3. A peripheral intraluminal filling defect that forms acute angles with the arterial wall .
Peripheral wedge-shaped areas of hyperattenuation that may represent infarcts, along with linear bands, have been demonstrated to be statistically significant ancillary findings associated with acute pulmonary embolism .
Chronic Pulmonary Embolism
The diagnostic criteria for chronic pulmonary embolism include .
(a) complete occlusion of a vessel that is smaller than adjacent patent vessels
(b) a peripheral, crescent-shaped intraluminal defect that forms obtuse angles with the vessel wall.
(c) contrast material flowing through thickened, often smaller arteries due to recanalization.
(d) a web or flap within a contrast material–filled artery .
(e) secondary signs, including extensive bronchial or other systemic collateral vessels , an accompanying mosaic perfusion pattern or calcification within eccentric vessel thickening .
Ancillary findings in chronic pulmonary embolism may include CT changes caused by pulmonary arterial hypertension: a pulmonary artery diameter greater than 33 mm.
Causes of Misdiagnosis of Pulmonary Embolism
Respiratory motion artifacts are the most common cause of indeterminate CT pulmonary angiography and can cause misdiagnosis of pulmonary embolism. These artifacts are best seen with lung window settings.
The low-attenuation abnormality due to partial volume averaging of vessel and lung can simulate pulmonary embolism.
Streak Artifact.—Beam-hardening streak artifacts from dense contrast material within the superior vena cava are commonly seen and can
overlie the right pulmonary and upper lobe arteries.This artifact can be distinguished from pulmonary embolism by recognizing its non anatomic, poorly defined, radiating nature.