



Internal cerebral vein (ICV) thrombosis
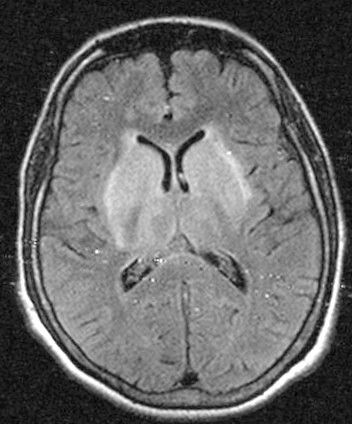
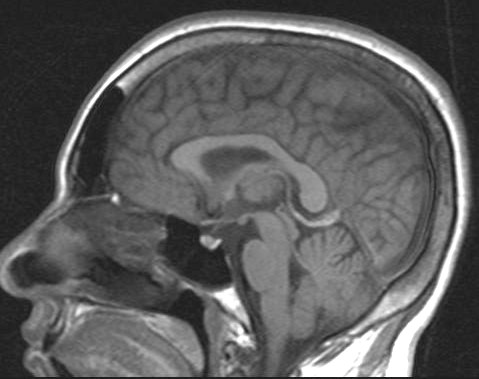
On MRI there is subacute thrombosis of the internal cerebral veins [T1 SAG] . Venous infarction with mild hemorrhagic transformation is seen in bilateral basal ganglia and thalami .
Etiology No cause identified on 20-25% of cases
- Trauma, infection (malaria) , inflammation
- Pregnancy, oral contraceptives
- Metabolic (dehydration, thyrotoxicosis, cirrhosis, etc)
- Hematological (coagulopathy)
- Collagen-vascular disorders (e.g., APLA syndrome)
- Vasculitis (e.g., Behcet)
- Drugs (androgens, ecstasy)
Imaging findings
CT Findings
- NECT
- Hyperdense vein = "cord sign"
- Parenchymal abnormality
- Thalami/basal ganglia appear hypodense with loss of GM/WM interfaces
- CECT
- "Shaggy," irregular veins (collateral channels) in deep WM, around tentorium.
- CTV
- Loss of ICV enhancement, presence of enlarged collateral channels.
MRI
- T1WI
- Clot: Early T1 isointense, later hyperintense
- Venous hypertension: Hypointense swelling of thalami, basal ganglia
- aVenous infarct: Hypointense edema, may be hemorrhagic
- Acute/early subacute clot: Peripheral enhancement outlines clot
- Late clot: Thrombus, fibrous tissue often enhances
- T2WI
- Clot: Often T2 hypointense mimicking flow void ("pseudo flow void"), much later hyperintense
- Venous hypertension: Hyperintense swelling of thalami, basal ganglia
- Corresponds to vasogenic edema
- Venous infarct: Parenchymal swelling, hyperintense edema, may be hemorrhagic
- MRV
- 2D time of flight (TOF) MRV shows "missing" ICVs, variable absent signal in V of G, SS
- May see abnormal collateral channels
- Contrast-enhanced MRV (CE-MRV)
- Faster; better depicts nonenhancing thrombus & small veins than TOF
- 2D time of flight (TOF) MRV shows "missing" ICVs, variable absent signal in V of G, SS
Angiography
- DSA more accurate than MRI
- Unlike quite variable superficial veins, deep cerebral veins are always present on angiography
Treatment
- Heparin +/- rTPA.
- Endovascular thrombolysis.